Genetic Female Hair Loss
Female pattern baldness is a type of hair loss that affects women. The first signs of female pattern baldness may be a widening part or a feeling that the hair does not feel as thick as usual. Although the scalp may be visible, the hairline usually does not recede.
Patterned hair loss, the most common type of hair loss affecting men and women, is characterized by a process of progressive hair miniaturization whereby large, pigmented terminal hairs are replaced by fine, colorless vellus hairs. In men, this condition preferentially affects hair on the superior and anterior temporal areas of the scalp, whereas in women it more commonly presents in a diffuse pattern in the crown, with or without sparing of the frontal fringe. 
The key point in patterned hair loss is progressive shortening of anagen phase. Since there is less time to grow, hairs become shorter and finer, to the point where individuals appear to be bald, despite the continuing existence of large numbers of fine vellus hairs.
Androgens play a central role in this process of miniaturization, hence the reason both male pattern hair loss (MPHL) and female pattern hair loss (FPHL) are collectively referred to as androgenic or androgenetic alopecia.
The Role of Androgens in Female Pattern Hair Loss
The influence of androgens in FPHL is not pronounced as in MPHL. Certainly, women with clinical hyperandrogenism- identified by the development of acne, hirsutism, and oligomenorrhea- frequently develop a pattern of hair loss similar to what is seen in males, with deep bitemporal recession and vertex thinning. However, the majority of women with FPHL shows no clinical signs of hyperandrogenism and have normal testosterone and dehydroepiandrosterone sulfate (DHEA-S) levels.
Genetic Factors
The mode of inheritance of FPHL is unknown. Women with FPHL have almost more than twofold male first degree relatives having with androgenic alopecia comparing to their female first degree relatives.
The Incidence and Degree of FPHL at Various Ages in Women
The incidence of female pattern hair loss (FPHL) is more difficult to establish than in men and its diagnosis are more challenging. This is because of less obvious patterns of hair loss than in men and because of the frequency with which other type of hair loss occurs. In brief, it is “the great mimicker” and should be included in the differential diagnosis of diffuse hair loss in any woman.
Three frequently occurring patterns of hair loss have been described in women:
A more or less “male pattern” or “fronto-parietal pattern”
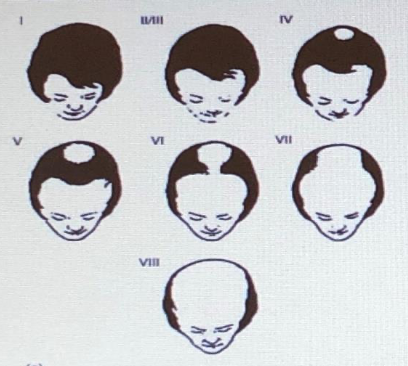
Hamilton examined 214 women in his study and found at least Type II MPB in 79% of them after puberty. He noted, however, that the bi-temporal recessions seen in Type II tended to be less prominent in women than in men and was likely to go unnoticed until their late twenties. Type IV MPB occurred in 25% of women by the age of 50 years and 50% had Type IV by the age 60 years. Type IV was defined as consisting of (i) deep fronto-temporal recessions extending more than 3 cm posterior to a coronal plane between the external auditory meatus and (ii) some mid-frontal hairline hair loss.
centrifugal pattern
A “centrifugal pattern” of hair loss first discussed by Ludwig: it consisted of hair loss over the caudal scalp. In contrast to Hamilton, he emphasized the essentially intact frontal fringe in these individuals. This type of hair loss arbitrarily divided in to three degrees of severity as shown in Fig. Postmenopausal women shoved an increased tendency to a more male pattern of hair loss.

Christmas tree
A “Christmas tree” pattern first described by Olsen (Fig. 2B2-5a and b). She noted that women with hair loss did not necessarily present with diffuse hair loss over the entire vaultal scalp, but instead may have increasing hair loss toward the frontal scalp “with encroachment on and sometimes breach of the frontal hair line”.

Medical Treatment Options & My Personal Way of Describing the Course of Medical Treatment
Before we start medical treatment, it’s very important that the patient is well informed about the course of this progressive-genetic hair loss/miniaturization, the length and frequency of the medical treatments; otherwise patients generally quit few months after the start of therapy mentioning that the therapy he/se has given was not effective and even might blame physician to be a trades man to sell therapies to the patients.
The best way to prevent misunderstandings and future problems regarding the effectiveness of the therapies that you have advised is thorough information.
So how I do it;
Description of FPHL in a simple way by giving the example of ‘water tank with a hole on the bottom’
We can assume the scalp like a tank filled with water with a hole on the bottom. Tank represents the scalp and the water in it represents the existing hairs. I tell my patients that, there exists a hole on the bottom of their tanks coming genetically where there is no way to close and continue telling that this hole’s size may vary accordingly to genetic tendency and their stress levels -which clears why the hair fall tends to peak time to time- and continue to tell that, their tanks will leak -more or less- all the time and best treatment to keep and increase the water level in this tank is keep adding water from outside. I also resemble the medical treatments like a fuel that we put in to our car’s tank where we need regular refueling. There is no miracle treatment which will cure the problem when applied few times thus you need to consider to seek the Dr’s advises during hair loss periods.

Hair Loss
Treatments
About Dr. Sezgin
Related Blog Posts
Results

HAIR TRANSPLANT IS ART AND SHOULD BE DONE BY ARTISTS!
Get a Consultation!
Find out if you are eligible for hair transplant surgery by using online consultation form below
With Dr. SEZGIN
Get a free consultation
Free Online Consultation
Please upload your images from sides, back, top, and front of your head as described by the pictures below.
Dr. Cagatay Sezgin
Burj Al Salam building 32nd floor Sheikh Zayed Rd, Dubai /UAE
+905326879626 Tue. – Sat. 10.00-17.00


